Conditions
Pancreatic Cancer
A comprehensive guide to understanding pancreatic cancer: from diagnosis and staging through treatment, surgery, recovery, and support.
On This Page
Understanding the Pancreas
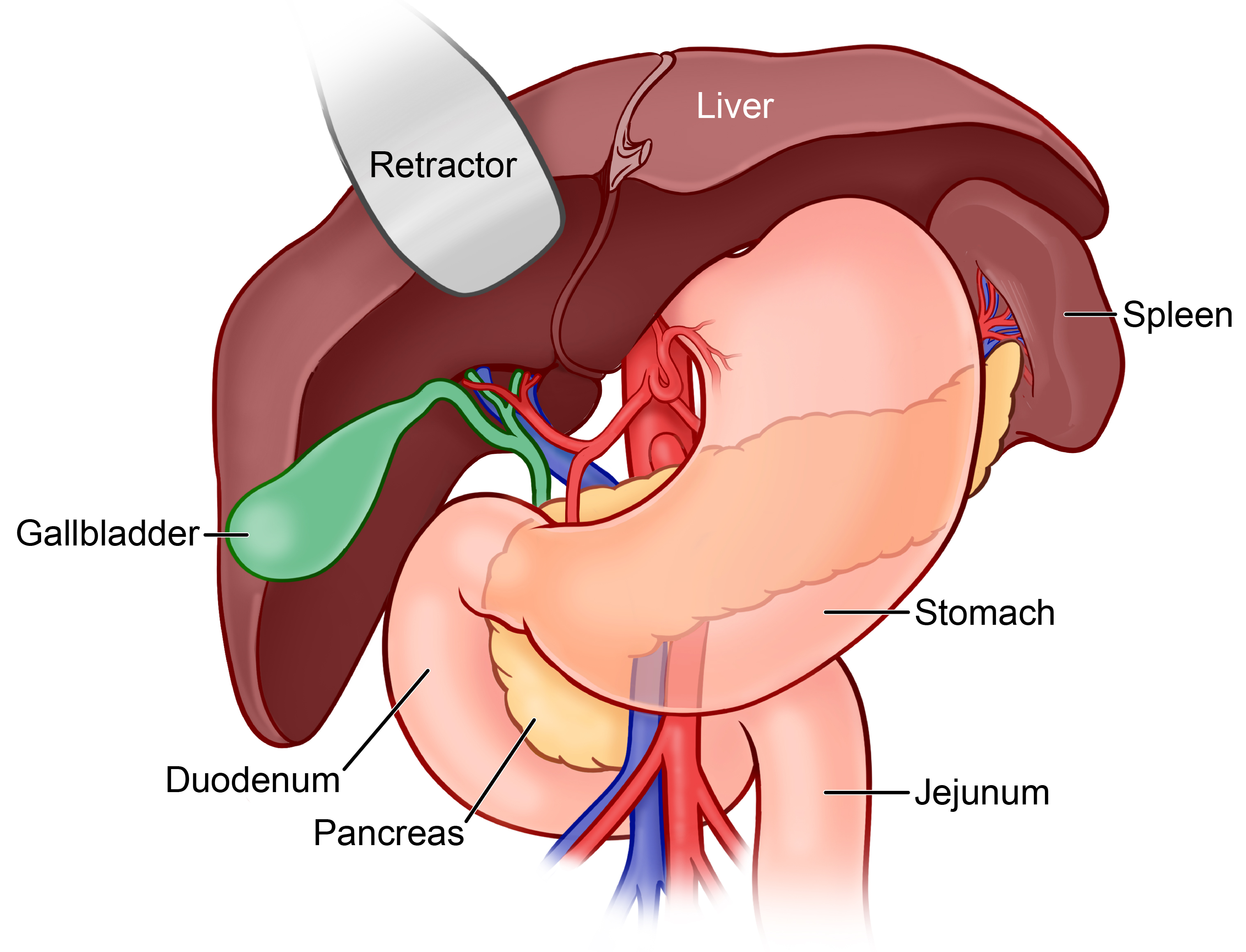
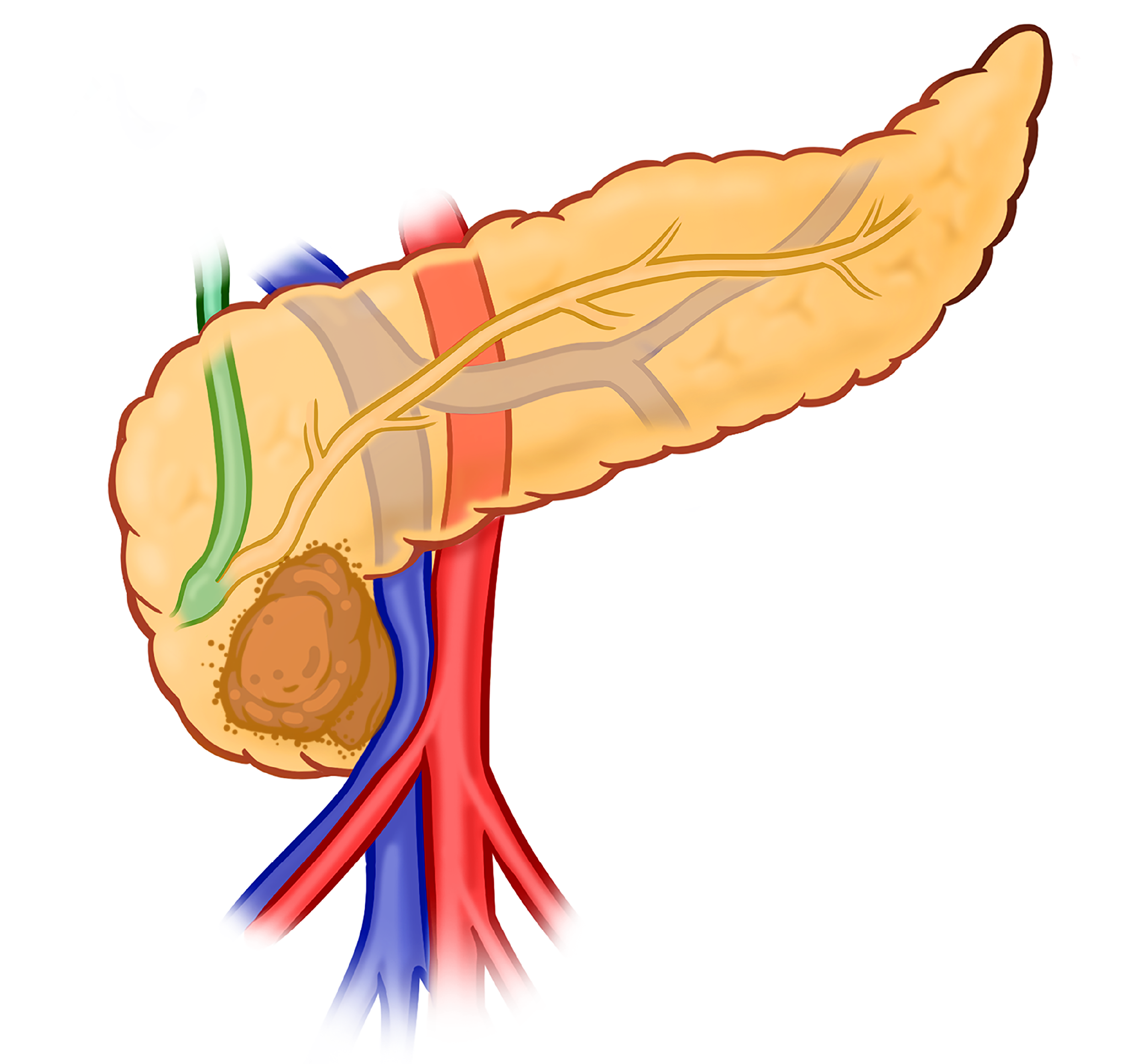
The pancreas is an organ located in the upper abdomen behind the stomach and colon, next to the spleen. It has two main jobs: regulating blood sugar through hormones like insulin, and producing digestive enzymes that break down fat, protein, and sugars. Anatomically it is divided into the head, neck, body, tail, and uncinate process, and is in close proximity to several major blood vessels supplying the liver, spleen, and intestines.
Exocrine Function
The exocrine pancreas produces digestive enzymes (lipase, amylase, and proteases) that are released through the pancreatic duct into the small intestine to break down fats, carbohydrates, and proteins. This function accounts for the vast majority of the organ by volume.
Endocrine Function
Scattered throughout the pancreas are clusters of cells called the islets of Langerhans, which produce hormones released directly into the bloodstream. The most important of these are insulin, which lowers blood sugar after meals, and glucagon, which raises it when levels fall, together maintaining stable blood sugar throughout the day.
Overview
What Is Pancreatic Cancer?
Pancreatic cancer is an abnormal, disorganized growth of cells that lose their normal function and replicate rapidly. It can invade neighboring organs and spread to other areas of the body. The most common type is adenocarcinoma; adenosquamous carcinoma and neuroendocrine tumors (PNET) are less common variants.
Potential Symptoms
- Painless jaundice (yellowing of skin or eyes)
- Pain in the abdomen and/or back
- Significant unexplained weight loss
- New-onset or worsening diabetes
- Low appetite, indigestion, or nausea
- Clay-colored, oily, or foul-smelling stools
Risk Factors
- Chronic or hereditary pancreatitis
- Family history of pancreatic cancer
- Smoking
- Long-standing diabetes
- Inherited gene mutations (BRCA1/2, PALB2, ATM, Lynch syndrome)
- Obesity and sedentary lifestyle
Pancreatic cancer is treated by a team of specialists: surgeons, medical oncologists, radiation oncologists, gastroenterologists, radiologists, pathologists, geneticists, social workers, and nutritionists. Consulting a high-volume specialist center leads to better outcomes.
Genetics
Genetic Considerations
About 1 in 10 cases of pancreatic cancer are inherited, passed down through families due to changes in DNA. Knowing your family history can help you understand your risks and take steps to protect your health.
What Is Genetic Testing?
Genetic testing looks at your DNA to find inherited changes that might raise your risk of pancreatic and other cancers. A simple blood or saliva test can help doctors find these changes and inform a plan for early detection and prevention. Genetic testing can also determine whether specific targeted therapies would be beneficial in patients with metastatic pancreatic cancer.
Who Should Be Tested?
It is strongly recommended that all patients with pancreatic cancer undergo genetic testing: both germline (inherited) and somatic (tumor) testing. A genetic counselor will guide you through the process and help you understand the results.
High-Risk Individuals
Screening & Surveillance
People with an elevated risk of pancreatic cancer may benefit from structured surveillance. Screening programs use annual MRI or endoscopic ultrasound (EUS) to detect early-stage tumors or precancerous lesions when they are most treatable.
Mount Sinai offers a dedicated high-risk pancreatic cancer surveillance program for eligible individuals. Enrollment is also available through an ongoing registry study.
Diagnosis
How Pancreatic Cancer Is Diagnosed
Once there is a suspicion of pancreas cancer based on imaging or other tests, a diagnosis is often confirmed by obtaining biopsies and other imaging studies that will help determine how advanced the cancer is, and guide treatment decisions.
Imaging
The primary tool for evaluating pancreatic cancer. Determines tumor size and location, vascular involvement, extension beyond the pancreas, and whether the tumor can be surgically removed. Special pancreas protocols are often necessary so your doctor might repeat a CT scan even if you had an initial screening scan to obtain additional detail. The test often involves IV contrast and takes about 15 minutes to perform.
A different kind of imaging study that uses magnets, not radiation. Particularly useful for evaluating the bile ducts, liver lesions, and cases where CT findings are unclear. It is also often performed with intravenous contrast and can take up to one hour to complete.
Specialized test that looks at how cells throughout the body use energy; typically, cancer cells use more and appear as bright spots. Used when CT or MRI results are unclear. Requires fasting; the process takes 2–3 hours total.
Tumor Markers
These are blood-based tests that are often elevated in the presence of malignancy. CA 19-9 is the primary blood test used to monitor pancreatic cancer; levels typically rise when cancer grows and fall when treatment is working. It is not diagnostic on its own, as it can be elevated in some non-malignant conditions and not every patient produces CA 19-9 so it can be normal even in the presence of confirmed cancer. CEA is a secondary marker used alongside CA 19-9, particularly in patients who do not produce CA 19-9.
Biopsy & Procedures
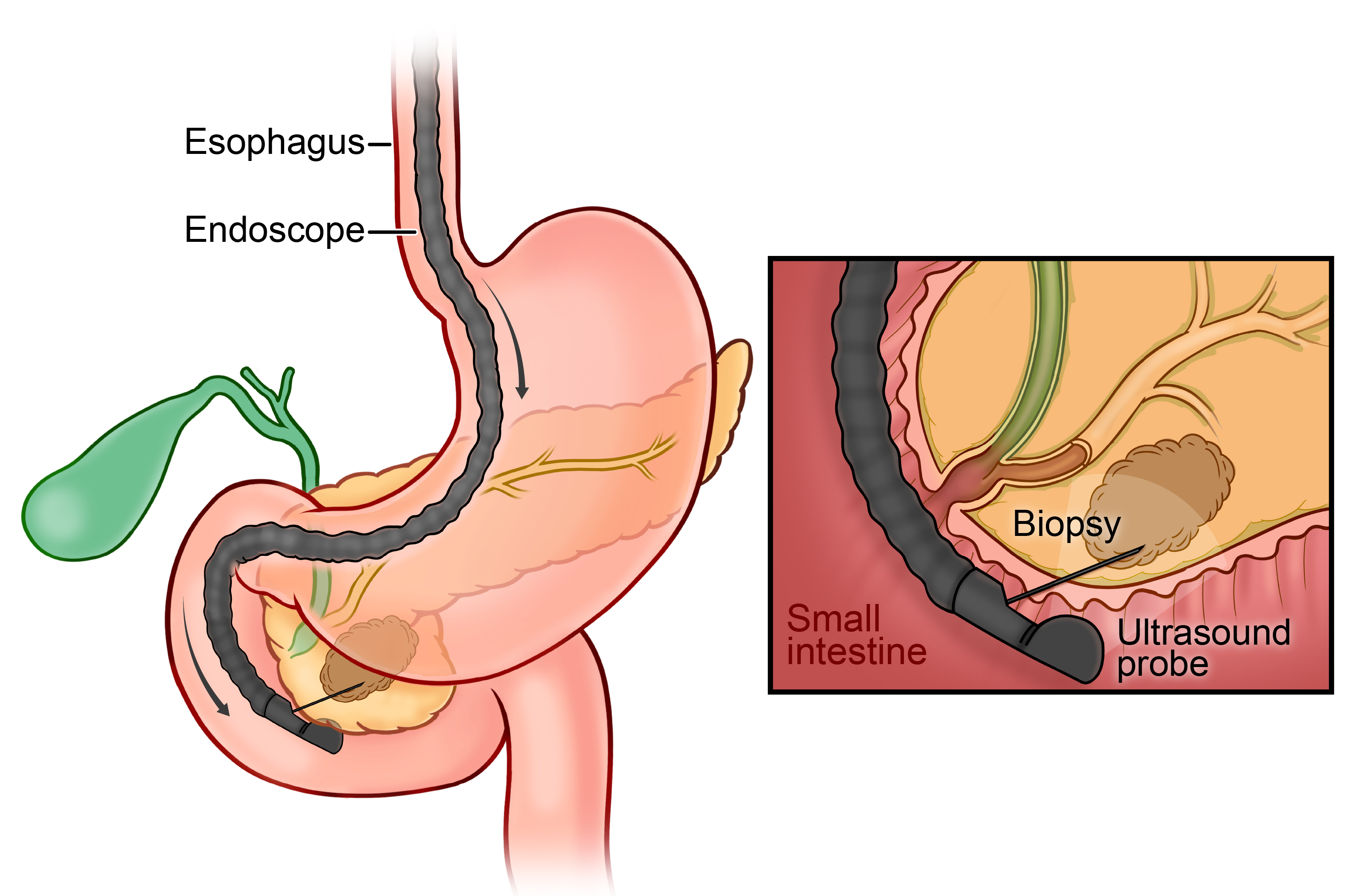
A thin flexible scope is passed through the mouth to image the pancreas up close and take a tissue sample with a fine needle. The sample is examined by a pathologist to confirm cancer type. Outpatient procedure; same-day discharge.
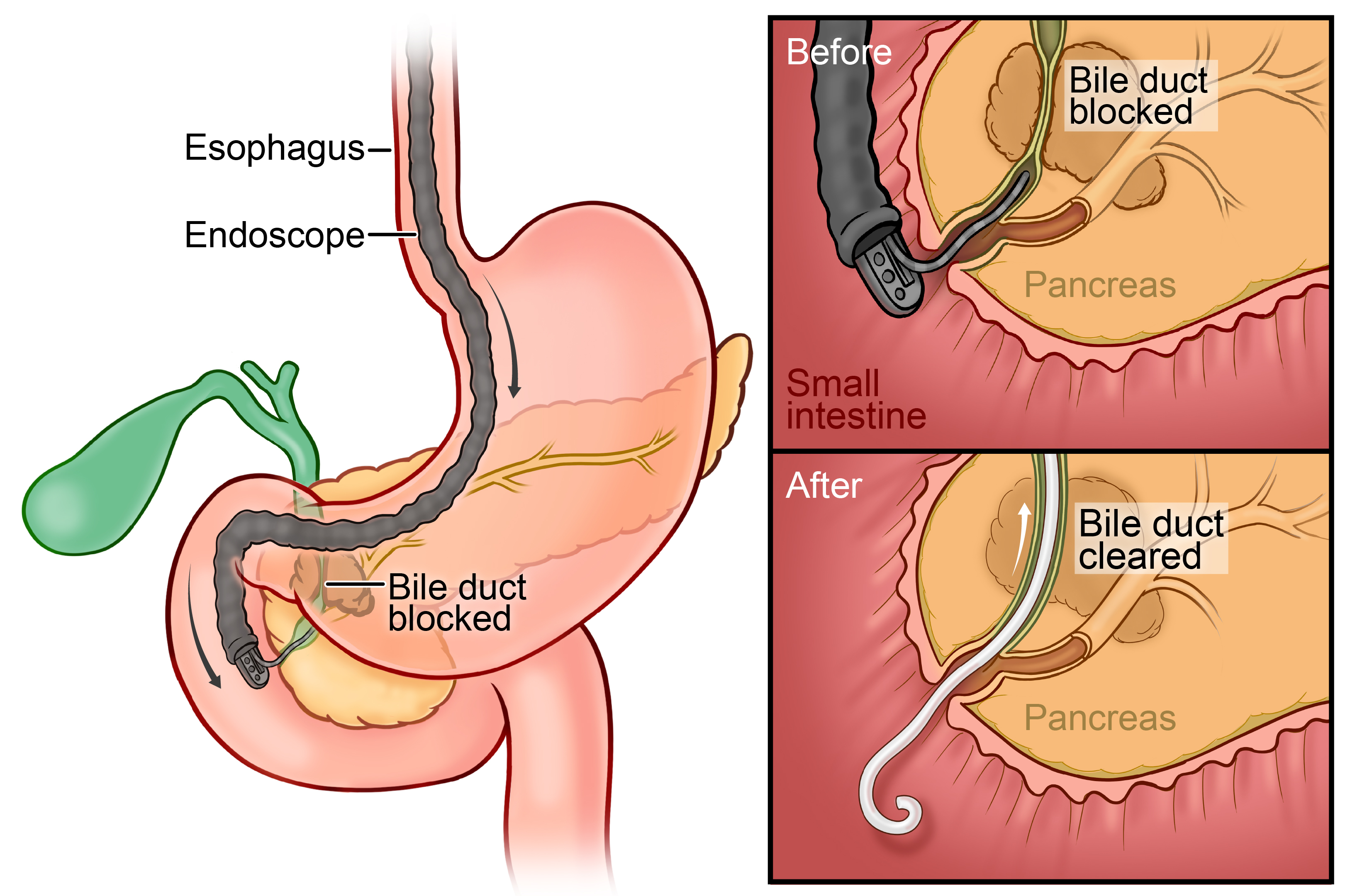
Used when a tumor blocks the bile duct, causing jaundice. A small stent is placed to restore bile flow. Often done in the same session as EUS; the EUS confirms the tumor and takes a biopsy while ERCP relieves the obstruction.
Important
A biopsy is required before starting chemotherapy or radiation. Patients going directly to surgery generally do not need one beforehand. Your team will determine the right sequence.
Staging
How Is Pancreatic Cancer Staged?
The most important initial question in staging is whether the cancer has spread to other organs or the lining of the abdomen (peritoneum). If distant spread is present, treatment focuses on systemic therapy. If it has not spread (stages I through III), patients may be candidates for a combination of systemic and local therapies, including surgery.
Note
In select situations, patients with limited metastatic disease who show a favorable response to chemotherapy may be considered for resection. This approach is generally offered as part of a clinical trial and is not standard practice.
CT, MRI, and PET scans determine the size and location of the tumor, whether it has grown into nearby blood vessels or organs, and whether it has spread to distant sites.
A short minimally invasive procedure where the surgeon looks directly at the liver and abdominal cavity for small deposits of cancer that may not appear on imaging. If hidden spread is found, major surgery is avoided and treatment is redirected to systemic therapy. Even when no visible disease is seen, fluid samples are taken from the abdomen to rule out microscopic peritoneal spread.
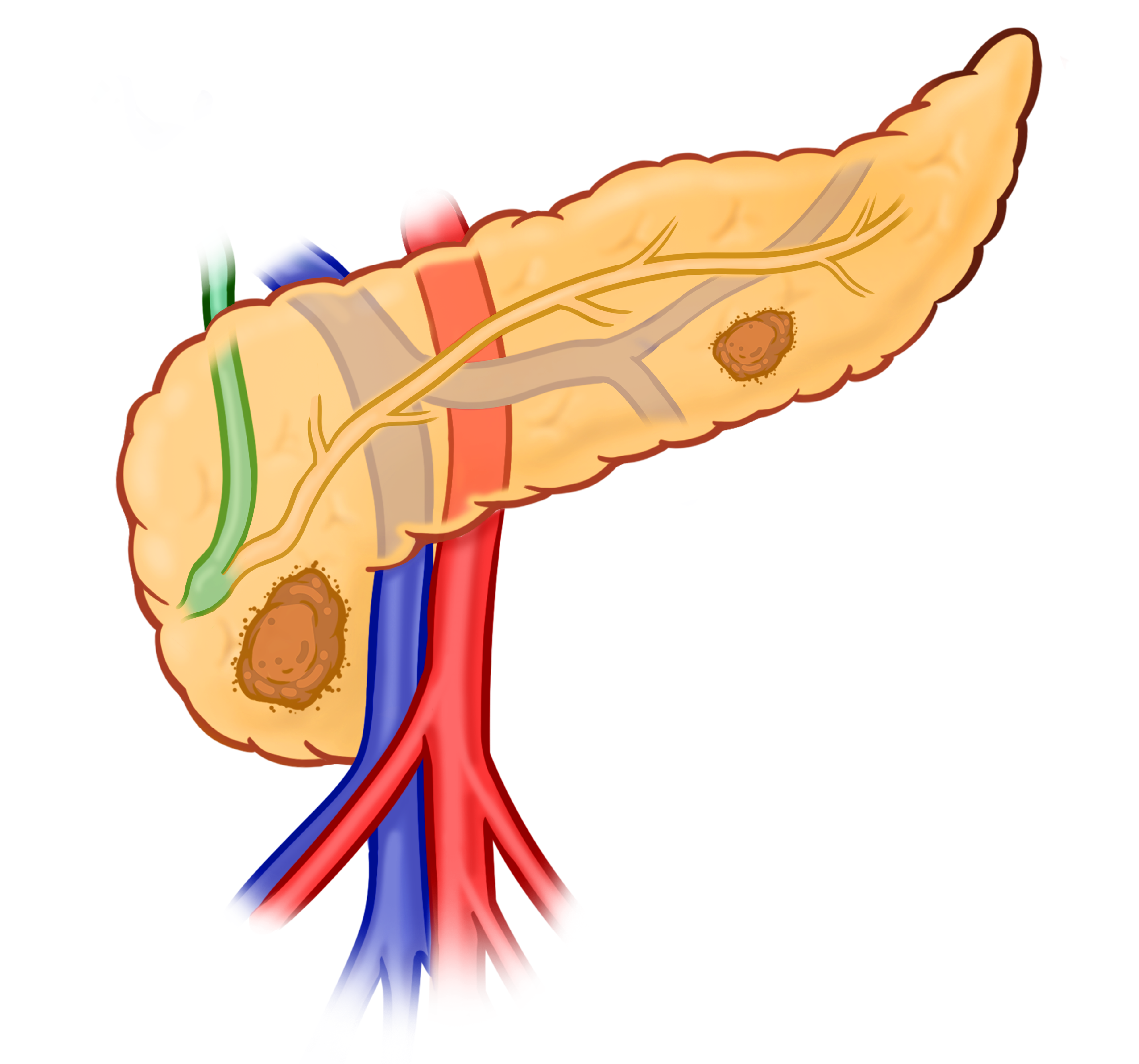
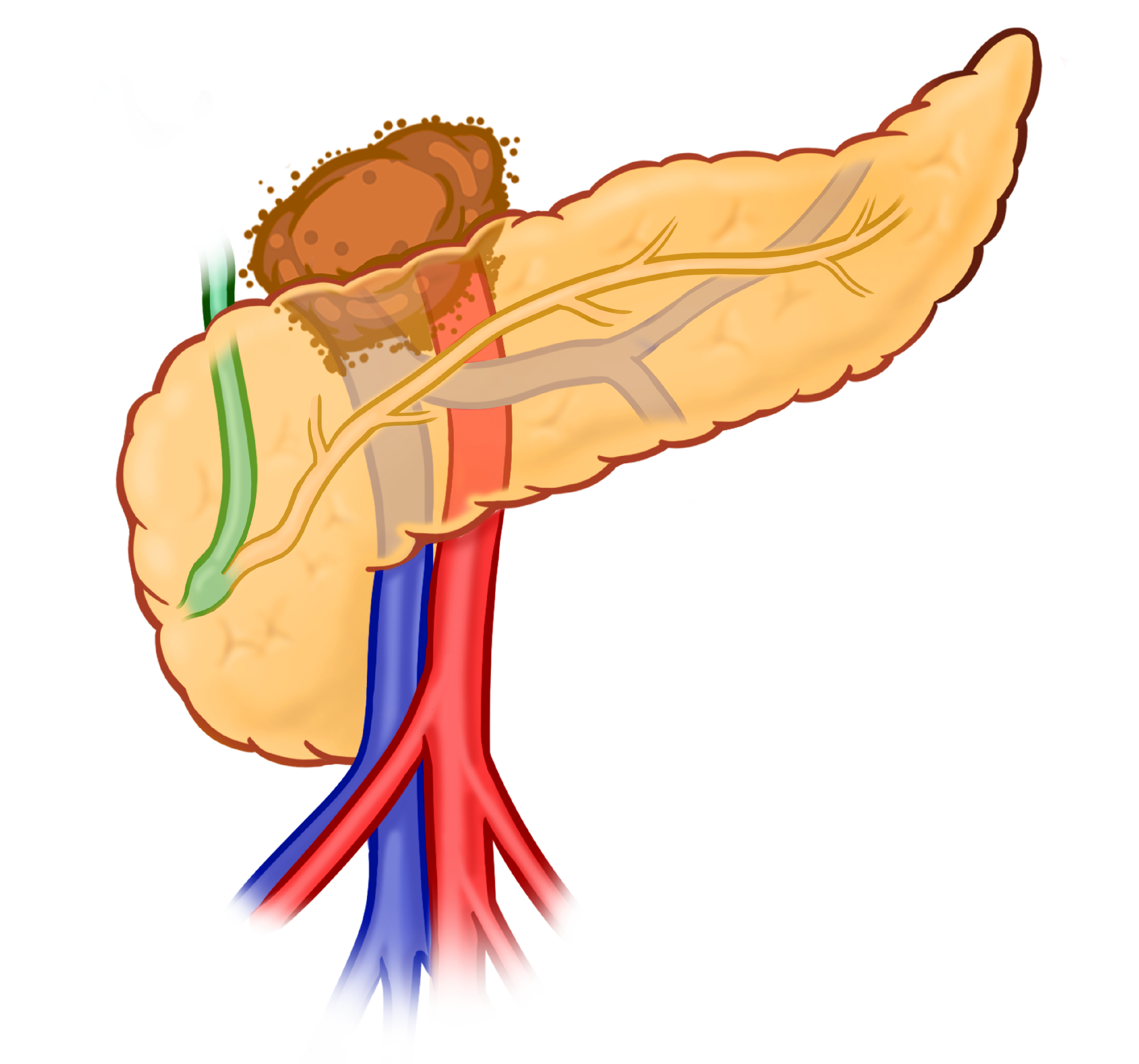
Resectability
Resectability refers to a surgeon's ability to completely remove a pancreatic tumor. Because these cancers frequently involve the blood vessels that pass directly behind and through the pancreas (including the superior mesenteric artery and vein and the portal vein), careful preoperative assessment is required. In many cases, vascular involvement can be addressed through resection and reconstruction at the time of surgery. In others, the extent of arterial encasement or multi-vessel involvement carries a risk that outweighs the potential benefit of an operation. This determination is best made by a surgeon experienced in hepatobiliary and pancreatic surgery, reviewing high-quality cross-sectional imaging in the context of the patient's overall condition.
Resectable
The tumor does not involve major arteries or veins. Surgery may be performed upfront or after neoadjuvant chemotherapy, depending on tumor biology and multidisciplinary team assessment.
Borderline Resectable
The tumor contacts and may distort (deform) major blood vessels without encasing them. Systemic chemotherapy is given first to improve the chance of a complete resection, which may require resection of major blood vessels with complex reconstruction.
Locally Advanced
Complex vascular involvement that cannot be safely reconstructed and precludes resection. Initial treatment is based on systemic chemotherapy, with radiation added in selected cases. Patients who demonstrate a favorable response and tumor biology may later be considered for surgery at specialized centers. It is important to plan ahead for possible surgery, as this may affect treatment planning.
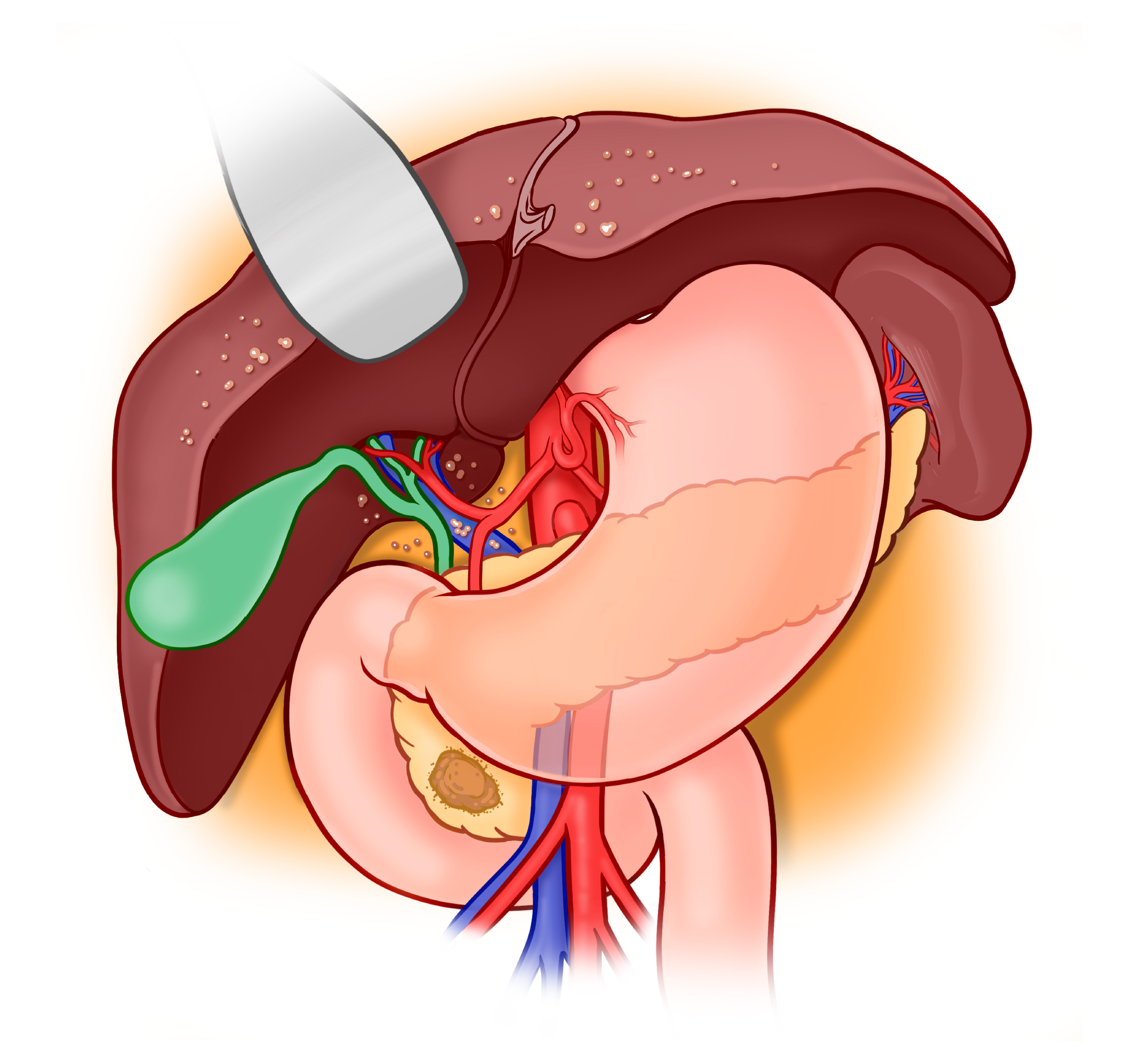
Metastatic Disease
Many patients present with metastatic disease at the time of diagnosis. This means that the tumor has spread from the primary tumor in the pancreas to other organs and implies stage IV disease. Most commonly this is seen in the form of liver metastases. In some cases there might be spread to the inner lining of the abdomen or the surface of abdominal organs; often this pattern of spread may not be detectable with radiographic studies and may require direct examination with laparoscopy (see staging laparoscopy); your team will discuss if this procedure is necessary in your case.
Clinical staging is based on imaging and pre-surgical exams. Pathological staging, based on what is seen under the microscope after surgery, can differ and provides more precise information. Accurate staging is essential because it determines the most effective sequence of surgery, chemotherapy, and radiation.
Treatment
Treatment Overview
Pancreatic cancer is treated with a combination of approaches tailored to each patient's stage, tumor location, and overall health. Treatment is planned by a multidisciplinary team and typically involves some combination of systemic therapy, surgery, and radiation.
Systemic Therapy
Chemotherapy, immunotherapy, and clinical trials. Systemic treatments travel through the bloodstream to target cancer cells throughout the body.
Learn more →Surgery
Whipple procedure, distal pancreatectomy, total pancreatectomy, and recovery. Surgery offers the best chance of cure for eligible patients.
Learn more →Radiation Therapy
High-energy X-rays targeted at the tumor. Used before surgery, after surgery, or to manage locally advanced disease.
Learn more →Supportive Care
Supportive Care
Treating the cancer is only part of the journey. Supportive care addresses nutrition, emotional well-being, and comfort throughout diagnosis, treatment, and beyond.
Nutrition
Managing weight loss, appetite, malabsorption, and enzyme replacement therapy during pancreatic cancer treatment.
Learn more →Social Work & Support
Coping strategies, advance care planning, and caregiver resources for patients and families.
Learn more →Palliative Care
Comfort, symptom management, and spiritual support throughout diagnosis, treatment, and beyond.
Learn more →FAQ
Frequently Asked Questions
Get an Expert Evaluation
Resectability assessments vary between centers. If you or a family member has been diagnosed with pancreatic cancer, or if told it is not operable, a second opinion is appropriate.